
The Anterior Cruciate Ligament (ACL) is an important ligament in the knee required for stability. If the ACL is injured, then you may have problems with the knee giving way on you, or you may have feelings of the knee being unstable.
Once the ACL has been injured then there is a high chance or risk that you may damage other structures in the knee such as articular cartilage (the cartilage that forms the lining of the knee joint), which may lead to early arthritis, and / or the meniscus (the piece of cartilage that sits between the two bones).
What is the Anterior Cruciate Ligament (ACL)?
- It is a ligament located in the middle of the knee.
- There are two main ligaments in the middle of the knee, the anterior cruciate ligament and the posterior cruciate ligament. It is called anterior because it is located anterior (in front) to the posterior cruciate ligament.
- A ligament is tissue that runs from one bone across a joint and connects with another bone.
- The purpose of a ligament is to provide stability on a joint.
- For the ACL that stability is to stop the tibia (leg bone) moving in front of the femur (thigh bone).
- The ACL also functions to limit rotation of the knee joint.
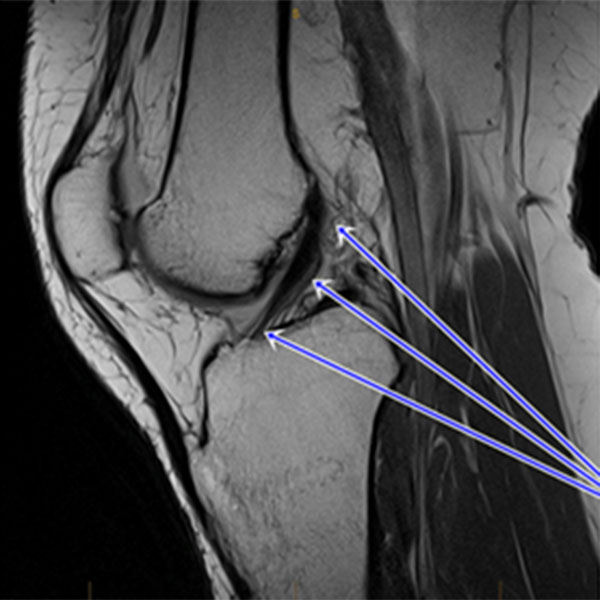
This is a MRI scan of the knee. The arrow is pointing to the anterior cruciate ligament (ACL). It runs from the back of the femur to near the front of the tibia.
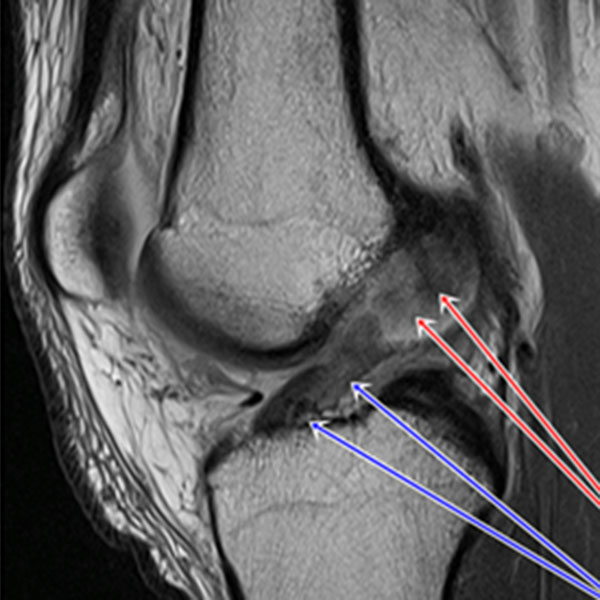
This MRI scan shows a ruptured anterior cruciate ligament. The easy to follow black structure (blue arrows) is completely missing at the top (red arrows).
How Does ACL Injury Occur
The ACL is most commonly injured whilst playing sports. It occurs when a force is applied to the knee that is greater than the ACL can handle and the ligament then ruptures.
It most commonly occurs with
- Twisting / turning (Pivoting)
- Contact
- Landing awkwardly from a leap or jump
- When the foot is planted to the ground
In Victoria the most common sports for injury are those that involve mechanisms where the knee is placed under stress. These include:
- Aussie Rules
- Netball
- Basketball
- Soccer
- Rugby
- Rugby League
- Martial Arts
- Snow sports
There are other ways that you can injure your ACL and these include:
- Motor vehicle accident
- Work injury
- A direct blow to the side of the knee
Symptoms
- Swelling: The most common symptom is swelling. This occurs because when the ACL ruptures, bleeding occurs into the knee joint. Swelling does vary and those that ice the knee straight away will have less swelling. The swelling tends to come up straight away (within the first couple of hours).
- Pain: The feeling of pain will be all around the knee initially.
- Sense of disruption: Patients commonly report that they felt as though “bones had moved” “my knee dislocated” “my knee was at a funny angle or position”.
- Patients will report (or those around them) – a snap or popping sensation.
- Patients generally speaking are not able to put weight on their knee (weight-bear) after an injury.
- If the injury occurs whilst playing sports, nearly everyone cannot continue playing.
- Those who have had an ACL reconstruction already, will report similar symptoms if they rupture their ACL graft.
There may be feelings of:
- Locking / catching (the meniscus or menisci could be damaged).
- Giving way / collapsing episodes (as the ACL is injured the stability of the knee is affected). It could also be due to a pain response.
Examination / Signs
- Effusion (swelling): This is normally moderate to large when the injury is seen within the first couple of weeks.
- Limp: Patients will walk with a painful limp - They may need crutches.
- Muscle wasting / weakness: The Quadriceps muscles (muscles at the front of the thigh) will start to lose thier bulk within 1 week of injury. This occurs because the knee joint is not being moved normally.
- Hamstrings tightness: The Hamstrings (muscles at the back of the thigh) may feel tight as they try to protect the knee. Some patients will not be able to get their knee out straight because of this.
Testing
Testing of the ACL is then performed. There are three tests that Nigel performs:
The Anterior Drawer
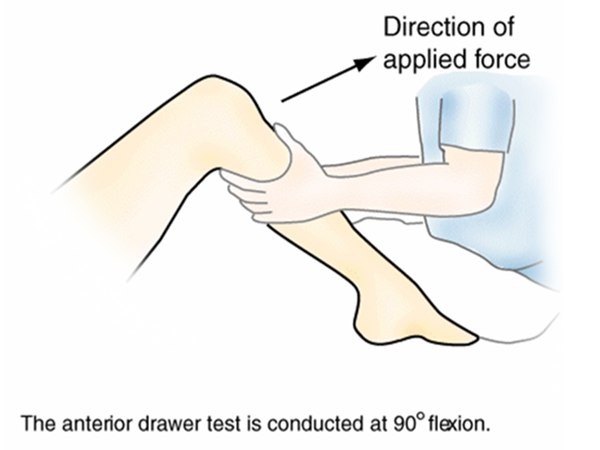
Nigel places your knee in 90° of flexion then pulls your leg forward.
The Lachmans Test
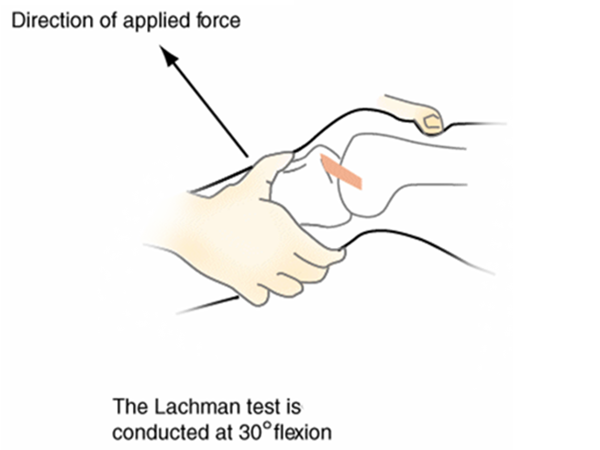
Nigel will then perform a test called the Lachman’s test. This is like the anterior drawer test but instead of the knee being bent to 90° the knee is flexed at 30°.
The Pivot Shift
The final test that Nigel will do for anterior cruciate ligament rupture is a test called the pivot shift. This test cannot always be done when you see Nigel because of pain and Nigel may only be able to perform this test in the operating theatre.
Nigel will also examine the rest of your knee to make sure that there are no other injuries to other structures in the knee. If there are and you require surgery Nigel will address those injuries when he reconstructs your ACL.
Structures that could be injured
Other ligaments
- Posterior cruciate ligament (PCL)
- Medial collateral ligament (MCL)
- Lateral collateral ligament (LCL)
- Posterolateral corner ligaments (PLC)
Other structures that could be injured
- Meniscal cartilage
- Medial (Inside)
- Lateral (Outside)
Investigations
X-rays may be done for the patient who seeks medical attention immediately after the injury to make sure there are no fractures. MRI scanning is considered to be the investigation of choice as it provides not only information on the ACL but also other structures in the knee that cannot be seen with x-rays.
Treatment
There are a number of different ways that ACL ruptures are treated initially.
- Protection
- Rest
- Ice
- Compression
- Elevation
Painkillers, and an anti-inflammatory should be used if able after seeking medical attention. The use of crutches should be encouraged initially. If bracing is going to be used, then a hinged knee brace should be utilised over a rigid knee brace.
Contacting a physiotherapist to start with simple quadriceps exercises and gentle range of movement is recommended. Medical advice should be obtained so that your injury is treated appropriately. This can be done by seeing your GP, sports medicine physician, or a physiotherapist.
A referral to Nigel can then be made and your knee will be assessed. If you wish to continue playing sport, have a heavy labour or high load occupation, have giving way, collapsing episodes, or instability with everyday activities then Nigel will recommend ACL reconstruction.
In a small minority of patients the ACL injured knee can undergo an intensive period of focused rehabilitation such that you may not require an ACL reconstruction.
Nigel in consultation with you, after listening to you, examining your knee, and reviewing all investigations will discuss with you the most appropriate treatment for your knee. You can ask any questions and if required a follow-up consultation can be made so that you can read all the information that is given to you.